Other Publications
Education Columns
Wellness Without Borders: Physician Wellness Programs in Family Medicine Practices in the United States vs Canada
By Rebecca Seekamp, MD, Stanford Family Medicine, Stanford Division of Primary Care and Population Health, Stanford, CA; Daniel Dodek, MD, Vancouver Division of Family Practice, Vancouver, BC; Traci Shiu, BS, Stanford Family Medicine, Stanford Division of Primary Care and Population Health, Stanford, CA; Cati Brown-Johnson, PhD, Evaluation Sciences Unit, Stanford School of Medicine, Stanford, CA; Eva Weinlander, MD, Stanford Family Medicine, Stanford Division of Primary Care and Population Health, Stanford, CA
This quality improvement project was funded by the Stanford Primary Care and Population Health Seed Grant.
INTRODUCTION
Physician burnout is a public health crisis, and family medicine is one of the most impacted specialties in both the United States and Canada.¹,² In 2023, a quality improvement (QI) project was undertaken to understand family medicine physicians’ experiences with wellness programs at Stanford Family Medicine and at the Vancouver Division of Family Practice.
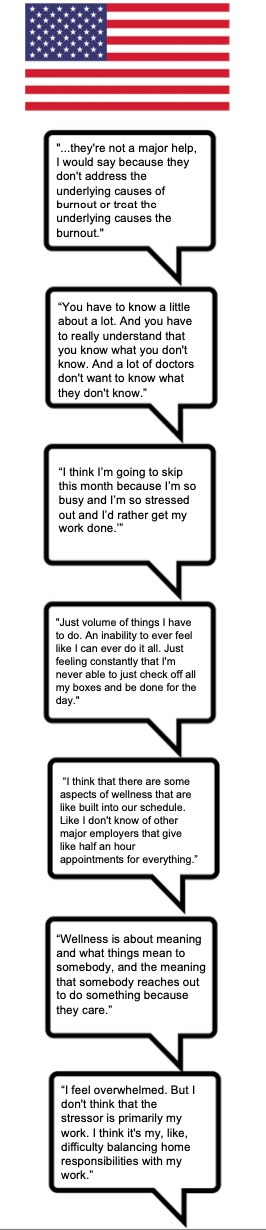
This QI project used a semi-structured interview guide consisting of open-ended questions about wellness programs at each institution. Interviews lasted approximately 60 minutes. The table below summarizes interview content by major theme.
Types of Wellness Programming
|
Program Type |
Stanford Family Medicine |
Vancouver Division of Family Practice |
|
Informal and Social Activities |
• Concert series |
• Weekend family social events |
|
Physical Wellness |
• Healthy Living program with individual health coaching |
• Individual physician exercise routines |
|
Mindfulness and Mental Wellness |
• Mindful meditation course, newsletter, and retreat |
• Mindfulness meditation retreat |
|
Work–Life Balance Support and Financial Wellness |
• Housing benefit |
• Locum support program |
|
Direct Peer Support |
• Commensality group dinners |
• Peer support initiative (pairing colleagues to discuss wellness or adverse events) |
- Dissonance Between Wellness Programs and Wellness Needs
Many physicians expressed cynicism toward institutional “wellness programs,” noting that these offerings do not address the core drivers of burnout—electronic health record (EHR) burden, administrative load, the complexity of family medicine, and persistent time pressure. - Stigma and Fear of Showing Weakness
Physicians reported reluctance to seek help, pursue mentorship, engage in coaching, or use mental health services. Interviewees described a pervasive medical culture of being “superhuman,” concern about stigma associated with mental health support, and fears about career consequences. - Barriers to Engagement
Wellness programs were often scheduled after clinic hours or on weekends, creating conflict with personal and family time. This timing was a major barrier to participation. - Connection and Sense of Belonging
Physicians consistently emphasized the importance of belonging to a trusted community. Those with supportive colleagues, teamwork, and safe spaces for clinical or personal discussion reported greater well-being. - Burnout and Moral Injury
Physicians described cumulative moral injury over recent years, contributing significantly to burnout. - Personal Identities and Wellness
Physicians described ongoing tension among their identities as clinicians, parents, spouses, and leaders. These domains intersect and influence overall wellbeing, making boundaries difficult to maintain.

DISCUSSION

Data from both institutions revealed shared themes in family physicians’ work and life experiences. We developed the concept of the “Wellness Iceberg” to visually represent physicians’ emotions, needs, and perceptions of institutional wellness efforts.
Above the waterline, physicians—especially those struggling—primarily see social gatherings and retreats. These can appear superficial and misaligned with their needs. Many organizational initiatives related to practice efficiency occur behind the scenes and progress slowly; because they are poorly communicated, they may be unknown, forgotten, or perceived as insufficient (eg, EMR working groups, adding nurses to teams, vacation coverage policies staffed by physicians with protected time, weekend in-basket coverage, lactation spaces/equipment, Circles Concierge, EHR elbow support).
Just below the surface are coaching and mindfulness programs, which are accessible, shareable, and supported by institutional resources. These programs can be beneficial, yet interviewees viewed them as secondary to deeper determinants of wellness.
The foundational elements—beneath the surface of the Wellness Iceberg—are the most important for sustaining well-being. Family physicians derive meaning from longitudinal relationships with patients. Many interviewees emphasized the critical role of compassionate leadership, supportive teams, and systems that restore a sense of control amid increasing demands and system-level challenges. Physicians who expressed fulfillment described trusting colleagues, strong teamwork, and meaningful friendships—connections that are central to thriving at work.
We began with the hypothesis that indicators of physician wellness would differ between the United States and Canada. However, interviews from Stanford Family Medicine and the Vancouver Division of Family Practice revealed a shared foundational need: human connection. Family physicians thrive when they have strong peer relationships and meaningful doctor–patient connections. Supporting these relationships requires innovative, compassionate leadership and a substantial reduction in administrative burden.
Physicians need less time in the EHR and more time engaging directly with patients and collaborating with colleagues. This shift is essential to restoring human connection in medicine, reducing burnout, and improving well-being.
Physicians also reported a mismatch between their needs and institutional interventions. Frequent, transparent, and psychologically safe communication between clinicians and leadership is necessary to bridge this gap. Effective leaders with the ability to connect meaningfully with clinicians are essential to ensuring that family physicians remain fulfilled and thriving.
- Buck K, Williamson M, Ogbeide S, Norberg B. Family physician burnout and resilience: a cross-sectional analysis. Fam Med. 2019;51(8):657-663. doi:10.22454/FamMed.2019.424025
- Canadian Medical Association. National Physician Health Survey 2021. Ottawa, ON: Canadian Medical Association; 2022. Accessed October 11, 2022. https://www.cma.ca/sites/default/files/2022-08/NPHS_final_report_EN.pdf
